Introduction

The American Heart Association (AHA) and American College of Cardiology (ACC) have released the 2026 dyslipidemia guidelines, introducing important updates in lipid management. These include a novel risk prediction model, more stringent lipid targets, and a stronger emphasis on early and personalized intervention.
Let’s break down the key takeaways in a simple, practical way.
Key Recommendations at a Glance
Screen Early
- Screening can begin as early as age 2 years in children with:
- Family history of premature ASCVD
- Severe hypercholesterolemia
- Familial hypercholesterolemia (FH)
- Universal screening is recommended at: 9–11 years
Check REGULARLY (Young Adulthood)
- Screen again at the age of 19 years
- Recheck every 5 years and use prevent ASCVD to assess risk
A New Risk Calculator: PREVENT™ Model
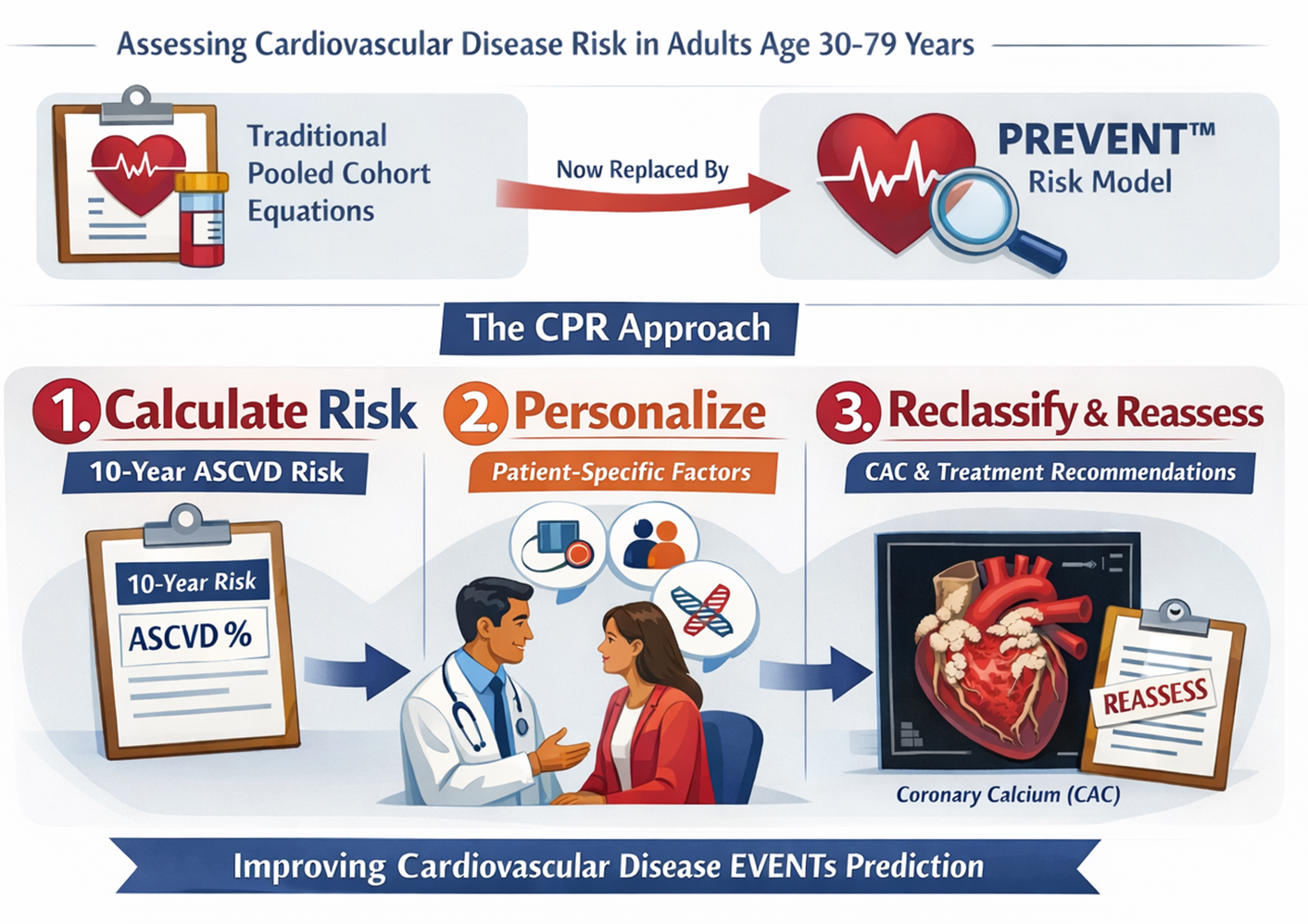
The traditional pooled cohort equations for 10- and 30-year risk assessment to guide lipid-lowering therapy in primary prevention in adults aged 30 to 79 years are now being replaced by the Predicting Risk of cardiovascular disease EVENTs (PREVENT™) risk model.
It follows a CPR approach:
- Calculate risk (10-year ASCVD risk)
- Personalize based on patient-specific factors
- Reclassify using tools like coronary artery calcium (CAC) and reassess treatment recommendations.
Act Early to Reduce Lifetime Risk
- Early identification ↓ prolonged exposure to atherogenic lipoproteins
- Lowers cumulative ASCVD risk over time
Lipoprotein(a)[Lp(a)]: Measure at Least Once
- Measure Lp(a) at least once in a lifetime to identify those individuals at higher risk of ASCVD
- High-risk thresholds:
- ≥50 mg/dL → 1.4-fold increased ASCVD risk
- ≥100 mg/dL → ≥2-fold higher estimated ASCVD risk
👉Elevated Lp(a) indicates the need for intensified LDL-C lowering and managing other risk factors.
Apolipoprotein B (ApoB): The “Better Marker” in Some Cases
- ApoB testing can improve risk assessment and guide therapy after LDL-C and non–HDL-C goals are met, especially in those with
- High triglycerides (>200 mg/dL)
- Diabetes
- Low LDL-C but persistent risk
👉 ApoB measurement helps identify adults with residual lipid-related risk that standard lipid profiles may underestimate and aids in diagnosing specific lipid and lipoprotein disorders.
Coronary Artery Calcium (CAC) – A Tool for Risk Refinement
- CAC scoring in men aged 40 and women 45+ improves risk assessment and guides LDL-C and non–HDL-C goals.
- Both CAC amount and standardized percentile (based on age, sex, and race) are prognostic and aid in reclassifying adult risk.
Treatment goals
- LDL-C and non–HDL-C goals resume guiding lipid-lowering therapy.
- Reducing LDL-C percentage remains a priority, with goals depending on ASCVD risk level.
- Consider early pharmacotherapy in Young Adults with
- Familial hypercholesterolemia
- LDL-C ≥160 mg/dL
- Strong family history of ASCVD
- Treat LONGER (Older Adulthood)
LDL-C Targets
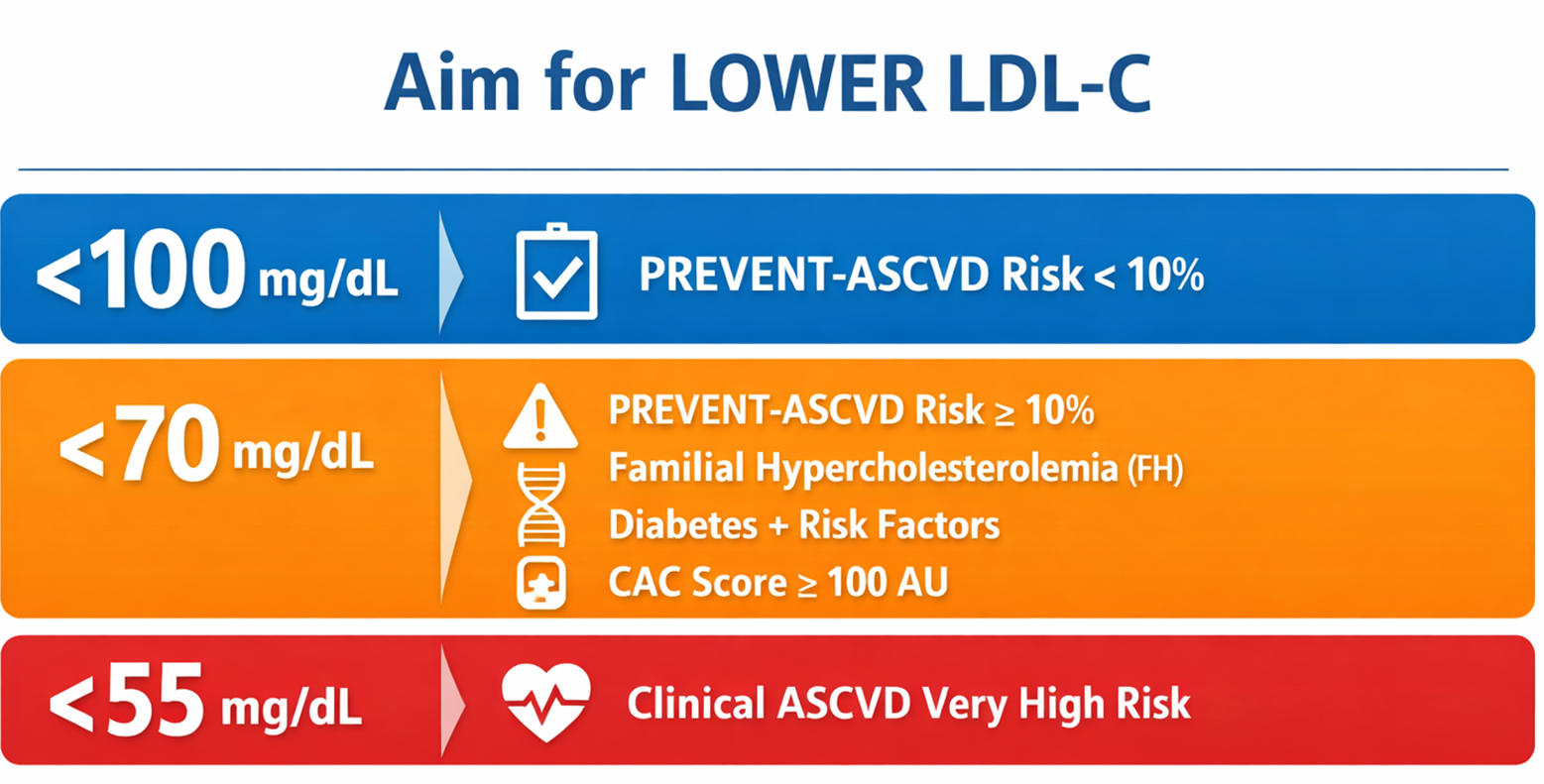
- <100 mg/dL
- Recommended for individuals with PREVENT-ASCVD risk <10%
- <70 mg/dL
- Recommended for individuals with: PREVENT-ASCVD risk ≥10%
- Familial hypercholesterolemia (FH)
- Diabetes mellitus with additional risk factors
- Coronary artery calcium (CAC) score ≥100 Agatston units
- Recommended for individuals with: PREVENT-ASCVD risk ≥10%
- <55 mg/dL
- Recommended for individuals with clinical ASCVD at a very high-risk
Start Lifestyle Measures Early
- Initiate health behavior counseling in youth
- Focus on:
- Heart-healthy diet
- Regular physical activity
- Weight optimization
Treat LONGER (Older Adulthood)
- Monitoring: Check lipids 4–12 weeks after starting or changing the dose of lipid-lowering therapy, then every 6–12 months thereafter.
- Duration: Benefits increase with longer therapy; tailor duration to individual risk.
LDL-Lowering Therapy: for Primary Prevention
- in adults without ASCVD with a 10-year PREVENT-ASCVD risk of:
- 3% to <5% (borderline risk)
- 5% to <10% (intermediate risk)
- regardless of baseline LDL-C levels for primary prevention in adults aged 40 to 75 years with:
- Diabetes
- Chronic kidney disease (stage 3 or 4)
- Human immunodeficiency virus (HIV)
- In adults aged >75 years, LDL-C–lowering pharmacotherapy may be considered alongside lifestyle interventions to reduce ASCVD risk.
Triglycerides Management
- Statins remain first-line therapy alongside lifestyle interventions in patients with persistently elevated triglycerides (TG) to reduce ASCVD risk
- severe hypertriglyceridemia: TG ≥1000 mg/dL
- Initiate TG-lowering therapies (omega-3 fatty acids, fibrates, and others)
- Primary goal → prevent acute pancreatitis
Conclusion
The 2026 dyslipidemia guidelines mark a shift toward earlier detection, personalized risk assessment, and more aggressive lipid lowering. By integrating tools like the PREVENT model and Lp(a) measurement, clinicians can better identify high-risk individuals. Ultimately, the goal is simple: reduce lifetime ASCVD risk through timely and targeted intervention.
Further Reading
- Wiggins BS, Barac A, Benziger CP, Blumenthal RS, Cibotti-Sun M, Moore M, et al. 2026 dyslipidemia guideline-at-a-glance. Journal of the American College of Cardiology. Published online 2026.https://www.jacc.org/doi/10.1016/j.jacc.2026.02.4872
- Blumenthal RS, Morris PB, Gaudino M, Johnson HM, Anderson TS, Bittner VA, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of dyslipidemia: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation.https://www.ahajournals.org/doi/10.1161/CIR.0000000000001423